Latest Obesity treatment drugs, research medication options along with what causes fatness and which food supplements can help you lose weight.
WHO fact files on obesity reveals that the condition has gone to epidemic proportions worldwide, with around 2.8 million deaths associated with being overweight or obese.
Obesity is a condition in which excess body fat has accumulated to such an extent that health may be negatively affected. It is commonly defined as a body mass index of 30 kg/m2 or higher. This distinguishes it from being overweight as defined by a BMI of 25 kg/m2 or higher.
Obesity or Excessive Weight is associated with various diseases, particularly e.g Cardiovascular Diseases, Diabetes Mellitus type 2, Obstructive Sleep apnea, Certain Types of Cancer and Osteoarthritis.
As a result, obesity has been found to reduce life expectancy. The primary treatment for obesity is dieting and physical exercise. If this fails, anti-obesity drugs and (in severe cases) bariatric surgery can be tried Obesity, in absolute terms, is an increase of body adipose tissue (fat tissue) mass. In a practical setting it is difficult to determine this directly. Therefore, obesity is typically assessed by BMI (body mass index)

Obesity Treatment Drugs, Causes and Research Medication
The first described attempts at producing weight loss are those of Soranus of Ephesus, a Greek physician, in the second century AD. He prescribed elixirs of laxatives and purgatives, as well as heat, massage, and exercise. This remained the mainstay of treatment for well over a thousand years.
It was not until the 1920s and 1930s that new treatments began to appear. Based on its effectiveness for hypothyroidism, thyroid hormone became a popular treatment for obesity in otherwise healthy people. It had a modest effect but produced the symptoms of hyperthyroidism as a side effect, such as palpitations and difficulty sleeping.
Dinitrophenol (DNP) was introduced in 1933; this worked by uncoupling the biological process of oxidative phosphorylation in mitochondria, causing them to produce heat instead of ATP. The most significant side effect was a dramatic rise in body temperature, frequently causing death. By the end of the 1930s DNP had fallen out of use.
Amphetamines (marketed as Benzedrine) became popular for weight loss during the late 1930s. They worked primarily by suppressing appetite, and had other beneficial effects such as increased alertness. Use of amphetamines increased over the subsequent decades, culminating in the “rainbow pill” regime. This was a combination of multiple pills, all thought to help with weight loss, taken throughout the day. Typical regimens included stimulants, such as amphetamines and thyroid hormone, diuretics, digitalis, laxatives, and often a barbiturate to suppress the side effects of the stimulants.
In 1967/1968 a number of deaths attributed to diet pills triggered a Senate investigation and the gradual implementation of greater restrictions on the market. This culminating in 1979 with the FDA banning the use of amphetamines, then the most effective of the diet drugs, in diet pills.
Meanwhile, phentermine had been FDA approved in 1959 and fenfluramine in 1973. The two were no more popular then other drugs until in 1992 a researcher reported that the two caused a 10% weight loss which was maintained for over two years.
Fen-phen was born and rapidly became the most commonly prescribed diet medication. Dexfenfluramine (Redux) was developed in the mid-1990s as an alternative to fenfluramine with less side-effects, and received regulatory approval in 1996.
However, this coincided with mounting evidence that the combination could cause valvular heart disease in up to 30% of those who had taken it, leading to withdrawal of Fen-phen and dexfenfluramine from the market in September 1997.
What are the Causes of Obesity and Fatness?
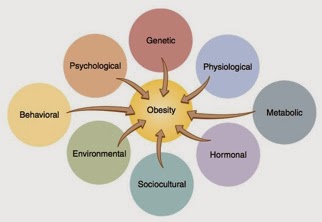
Most researchers agree that a combination of excessive calorie consumption and a sedentary lifestyle are the primary causes of obesity. In a minority of cases, increased food consumption can be attributed to genetic, medical, or psychiatric A 2006 review identifies ten other possible contributors to the recent increase of obesity.
- Insufficient sleep
- Endocrine disruptors—food substances that interfere with lipid metabolism
- Decreased variability in ambient temperature
- Decreased rates of smoking as smoking suppresses appetite
- Increased use of medication that leads to weight gain
- Increased distribution of ethnic and age groups that tend to be heavier
- Pregnancy at a later age
- Positive natural selection of people with a higher BMI
- Genetic factors
- Lack of Physical activity
- Intake of Weight gaining substances like creatin
Anti-obesity or weight loss programs contains two main constituents as given below:
- Obesity treatment without drugs using non therapeutic obesity treatment programs
- Obesity treatment with drugs using therapeutic obesity treatment programs
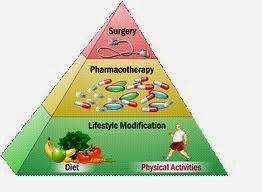
Obesity Treatment without Supplements, Drugs or Medications
Obesity treatment without drugs using non therapeutic obesity treatment programs includes weight loss techniques without using medications:
- Exercise for Obesity treatment
Regular exercise is very important for diabetic as well as obesity patient. Actually exercise works as calorie burner as well as metabolism booster. Both of these effects play very important role in reducing body fat by consuming excessive storage depots of fats. - Diet for Obesity treatment
Diet is another non therapeutic way to reduce body weight and to treat obesity. Actually by restricting your diet from fatty food and constituents that contains high amount of calorie like sugar will help you to limit your body fat reservoirs.
Obesity Treatment with Drugs
For hard to treat patient, obesity treatment with drugs using therapeutic obesity treatment programs. Therapeutic treatment includes Obesity treatment drugs, medications and supplements that specifically target obesity by different mechanisms. These medications are given below:
-
Sibutramine for Obesity Treatment
Sibutramine (Reductil or Meridia) is an anorectic or appetite suppressant, reducing the desire to eat. Both drugs have side effects. Sibutramine may increase blood pressure and may cause dry mouth, constipation, headache, and insomnia.
-
Metformin for Obesity Treatment
In people with Diabetes mellitus type 2, the drug metformin (Glucophage) can reduce weight.
-
Byetta for Obesity Treatment
Byetta (Exenatide) is a long-acting analogue of the hormone GLP-1, which the intestines secrete in response to the presence of food. Among other effects, GLP-1 delays gastric emptying and promotes a feeling of satiety. Some obese people are deficient in GLP-1, and dieting reduces GLP-1 further. Byetta is currently available as a treatment for Diabetes mellitus type 2. Some, but not all, patients find that they lose substantial weightwhen taking Byetta. Drawbacks of Byetta include that it must be injected twice daily, and that it causes severe nausea in some patients, especially when therapy is initiated. Byetta is recommended only for patients with Type 2 Diabetes. A somewhat similar drug, Symlin, is currently available for treating diabetes and is in testing for treating obesity in non-diabetics.
-
Symlin for Obesity Treatment
Symlin (Pramlintide) is a synthetic analogue of the hormone Amylin, which in normal people is secreted by the pancreas in response to eating. Among other effects, Amylin delays gastric emptying and promotes a feeling of satiety. Many diabetics are deficient in Amylin. Currently, Symlin is only approved to be used along with insulin by Type 1 and Type 2 diabetics. However, Symlin is currently being tested in non-diabetics as a treatment for obesity. A drawback is that Symlin must be injected at mealtimes.
-
Rimonabant for Obesity Treatment
Recent pharmaceutical research has produced potential obesity combating drugs. The discovery of cannabinoid receptors in the brain, liver and muscle has stimulated research in a new class of drugs, namely cannabinoid (CB1) receptor antagonists. These drugs not only causes weight loss, but prevent or reverse the metabolic effects of obesity, such as insulin resistance and hyperlipidemia, and may also decrease the tendency to abuse substances such as alcohol and tobacco.
Orlistat: Obesity Treatment Research Medications
Orlistat is the only non-controlled anti-obesity prescription drug approved by FDA. Obesity refers to an excessive amount of body fat. Most health care professionals agree that men with more than 25 percent body fat and women with more than 30 percent body fat are obese.
Most available weight-loss medications approved by the Food and Drug Administration (FDA) are appetite-suppressant medications. However, Orlistat is one drug that works in a different way. Orlistat works by reducing the body’s ability to absorb dietary fat by about one third. It does this by blocking the enzyme lipase, which is responsible for breaking down dietary fat. When fat is not broken down, the body cannot absorb it, so fewer calories are taken in.
Prescription weight-loss medications should be used only by patients who are at increased medical risk because of their weight. They should not be used for “cosmetic” weight loss. Prescription weight loss drugs are approved only for those with a body mass index (BMI) of 30 and above, or 27 and above if they have obesity-related conditions, such as high blood pressure, dyslipidemia (abnormal amounts of fat in the blood), or type 2 diabetes. BMI is a measure of weight in relation to height. A BMI of 18.5 to 24.9 is considered healthy.
Orlistat Dosage and Administration
The recommended dose of orlistat is one 120 mg capsule three times a day with each main meal (during or up to one hour after the meal). Orlistat is currently approved for use in teens age 12 or above.
Orlistat Mechanism for Weight Loss
Orlistat works by inhibiting pancreatic lipase, an enzyme that breaks down triglycerides in the intestine. Without this enzyme, triglycerides from the diet are prevented from being hydrolyzed into absorb-able free fatty acids and are excreted undigested. Only trace amounts of orlistat are absorbed systemically; the primary effect is local lipase inhibition within the GI tract after an oral dose. The primary route of elimination is through the feces.
Orlistat Trials Results for Obesity Treatment
The amount of weight loss achieved with orlistat varies. In one-year clinical trials, between 35.5% and 54.8% of subjects achieved a 5% or greater decrease in body mass, although not all of this mass was necessarily fat. Between 16.4% and 24.8% achieved at least a 10% decrease in body mass. After orlistat was stopped, a significant number of subjects regained weight—up to 35% of the weight they had lost.
For further learning please watch our video on Obesity Causes,Types,Treatment, and Symptoms!
[youtube id=”Q03bO3b78yA”]